
CT of Non-traumaticAcute Aortic Disease
Mindy M. Horrow, MD, FACR
Director of Body Imaging
Albert Einstein Medical Center
All photos retain the copyrights of their original owners
© Mindy Horrow, MD
Outline
Introduction
Imaging Techniques
Classic Aortic Dissection
Intramural Hematoma
Penetrating Atherosclerotic Ulcer
Complications
Introduction
Acute aortic dissection is most common aorticemergency
Helical CT with sensitivity and specificity near100%
Considered acute if sx < 2 weeks, chronic if longer
75% deaths occur within 2 weeks of initial sx
Hypertension is major cause adding mechanicalstress to aortic wall with longitudinal shearingforces and decreased vasa vasorum flowincreases stiffness of media causing more stressand contributing to development of dissection
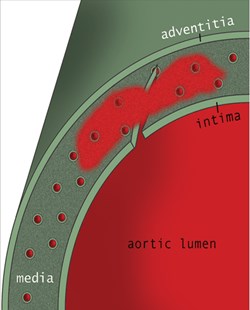
Tear of aortic intima and inner layer aortic media allowingblood to split the media. Forms double channel with flapcomposed of intima and inner media. Re-entrance tearscreate additional communications between true and falselumens.
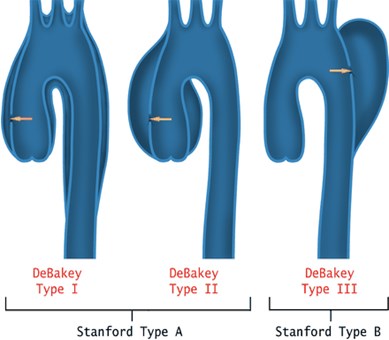
Classification systems: DeBakey, superseded by Stanford inwhich 2 types are based upon whether surgery is required.
–Stanford A- dissection involving ascending aorta or arch
–Stanford B-dissection begins distal to left subclavian artery
Treatment according to Type ofDissection
Acute A dissection requires immediate repairto avoid extension into pericardium, pleuralspace, coronary arteries or aortic valvular ring
Chronic A dissection, usually associated withabnormalities of the ascending aorta such ascystic medial necrosis, also requires surgery
Type B dissection treated medically unlesscomplications occur: organ ischemia orpersistent pain
Imaging Technique
Unenhanced scans to detect intramuralhemorrhage (5mm collimation from 3 cmabove aortic arch to bifurcation)
Enhanced scans: 3-4 mL/sec bolus (rightarm preferred to avoid artifact from LBrachiocephalic vein), pitch 1.5 recon to1.25mm sections on 4 slice scanner, 1mmon 16 slice. Use Smart prep or 25 secdelay. Scan 3 cm above arch tobifurcation of iliac arteries
Typical Aortic Dissection
Unenhanced CT- internal displacement ofintimal calcifications which can beconfused with calcified mural thrombus.Look for high attenuation of false lumen
Enhanced CT- intimal flap, (1)differentiation of true from false lumen,(2) differentiation of aortic aneurysm withintraluminal thrombus from dissectionwith thrombosed false lumen
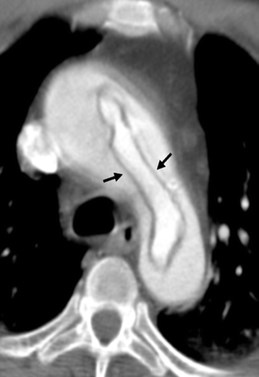
18 year old with history of congenital heart disease
Intimal flap visible because of anemia
Coarctation of the Aorta
Castaner
Differentiation of True from FalseLumen
Lumen in dissected portion that iscontinuous with lumen of undissectedportion of aorta is true lumen.
If lumen ends in blind sac, it is falselumen
If one lumen completely surrounds otherlumen, inner one is true lumen
Occasionally difficult to be sure if lumensare blurred in aortic root
True inner lumen of aortic archcompletely surrounded byfalse lumen= intussception ofintimal flap
Classic appearance of intimalflaps in ascending anddescending aorta
Castaner
Differentiation of True from FalseLumen
Beak sign: acute angle betweendissection flap and outer wall, spaceformed by acute angle could be filled withcontrast enhanced blood or hematoma.MOST USEFUL SIGN
Eccentric flap calcification-seen on truelumen side
Outer wall calcification- only of truelumen in acute cases, occ in false lumenwhen chronic dissection present
Lepage, etal AJR;177:207-211
Differentiation of True from FalseLumen
Cobwebs- thin, linear radiolucent defectsin lumen attached to wall at one end.Represent ribbons of media incompletelysheared off by dissection. Specific, butnot sensitive for false lumen
Intraluminal thrombus more common infalse lumen, especially in chronic cases
False lumen usually larger than true withflap straight or curved towards falselumen
Lepage, etal AJR;177:207-211

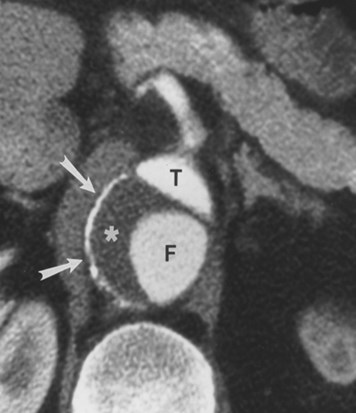
Acute Dissection:
Flap curvedtowards falselumen, with beaksign in larger, falselumen
LePage

Type B dissection with cobweb sign in false lumen, whichalso shows beak sign. Smaller true lumen
Castaner

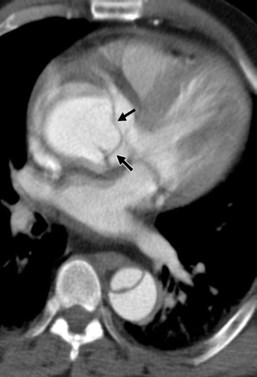
AcuteDissection:
Flap curvedtowards truelumen with smallamountthrombus in“beak” of falselumen
LePage
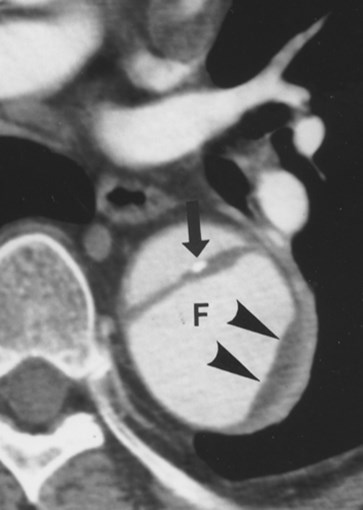
ChronicDissection:
Flat dissection flapwith eccentriccalcification alongtrue lumen side offlap.
False lumen islarger andcontains thrombus
LePage
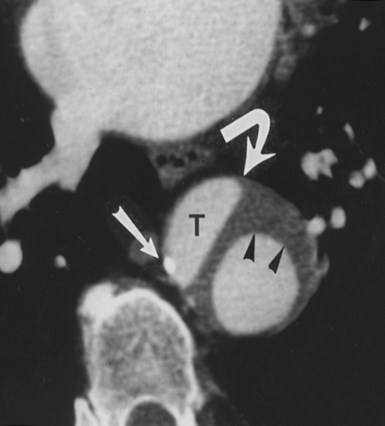
Chronic Dissection:
Outer wallcalcification in truelumen, thrombus infalse lumen beak
LePage
ChronicDissection:
Outer wallcalcification andthrombus in falselumen
LePage
Intramural Hematoma
Caused by spontaneous hemorrhage ofv. vasorum which weakens media withoutan intimal tear
13% Acute aortic dissections
Similar clinical manifestations and risksto typical a. dissection
Use Stanford Classification
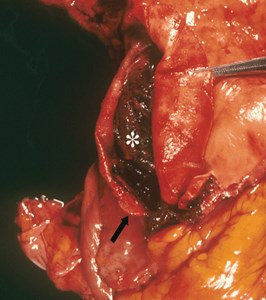
Intramural Hematoma
Rupture of vasa vasorumleads to bleeding within aorticmedia and intact intima
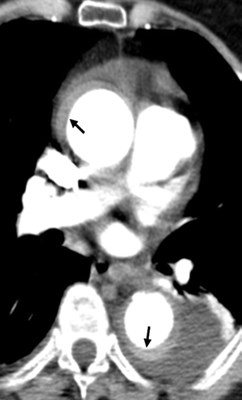
IMH Non-Contrast CT
Crescent shaped area of differentattenuation in aortic wall.
May not compress aortic lumen
Intimal calcifications may bedisplaced
Contrast from enhanced CT mayobscure IMH
IMH Contrast CT
Crescent of IMH does not enhance
Tends not to spiral as would thethrombosed lumen of a typical dissection
Relationship to typical dissection unclear
Progression to typical dissection morelikely if Type A IMH, thick hematomacompresses true lumen, pericardialeffusion

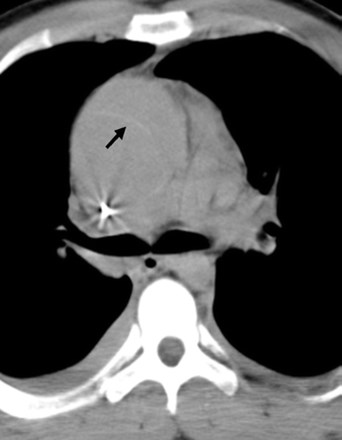
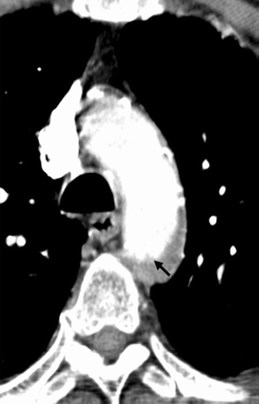
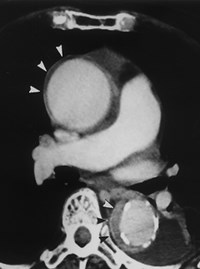
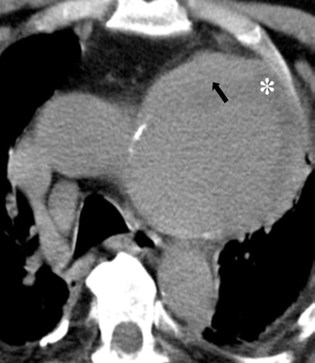
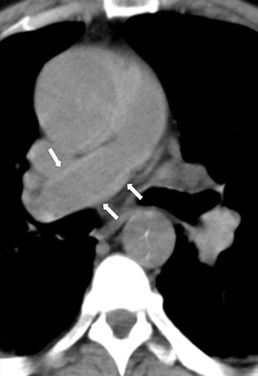
Type A IMH: high density crescents, displaced intimal
Calcifications, no enhancement after contrast (less obvious)
Castaner
Castaner
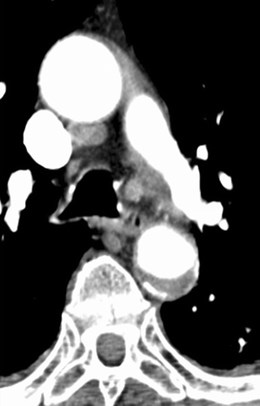
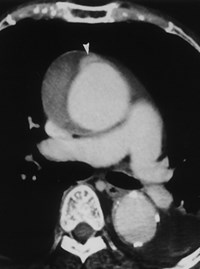
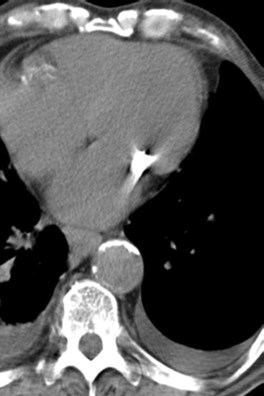
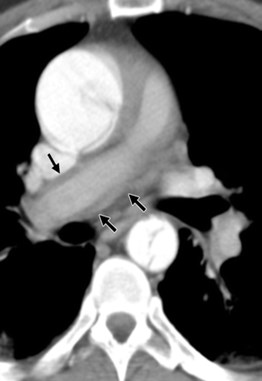
Mural thrombus with irregular border, overlies calcified
Intima and maintains a constant location in aorta
Castaner
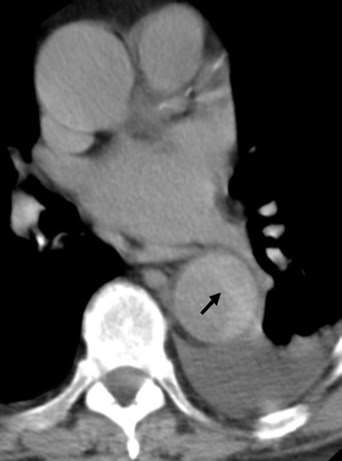
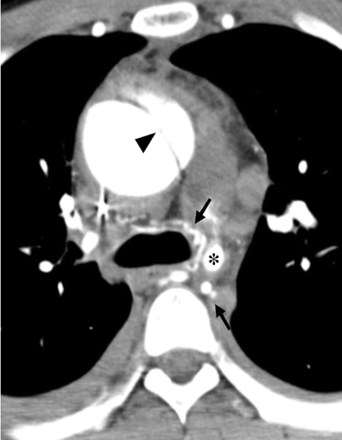
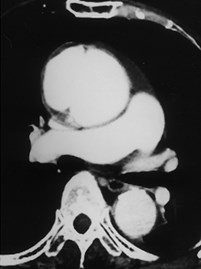
Type B IMHcompressinglumen with pleuraleffusion.Findings increaselikelihood ofprogression todissection
Castaner

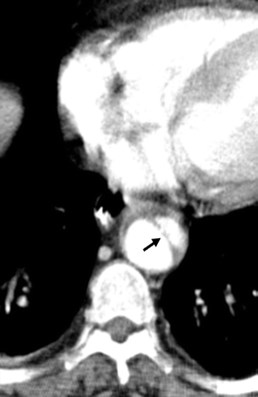
Evolution of IMH to frank dissection one week later
Castaner
Initial Type A IMH, 2 days later larger IMH with ulcer, 3 months later showsenlargement of ulcer, required surgery
Type A IMH has higher incidence of these ulcers than Type B
Sueyoshi
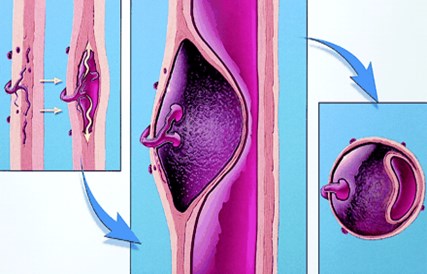
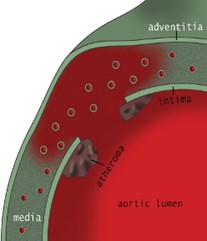
Penetrating Atherosclerotic Ulcer
Ulceration of atheromatous plaque thaterodes inner, elastic layer of aortic walland when it reaches medial layer media isexposed to arterial flow, causinghemorrhage in wall. Localized dissectioncan occur, break into adventitia, resultingin PSA or rupture
Penetrating Atherosclerotic Ulcer
May result in aneurysms, particularlysaccular type
Often occur in elderly withatherosclerosis
Typically involve arch and descendingaorta



1
2
3
4
CT Findings
Unenhanced: extensive atherosclerosis, focaland variable IMH, displaced intimalcalcification
Enhanced: Collection of contrast visualizedoutside lumen, similar to peptic ulcer. May bemultiple or single with thickening of aorticwall. Atheromatous ulcers confined to intimamay be seen in asymptomatic patients, butshould be followed for progression to aorticaneurysm. When rupture occurs, impossibleto differentiate from ruptured aneurysm.
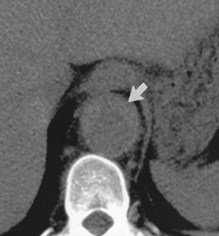

Unenhanced CT with IMH, enhanced CT atsame level shows ulcer filled with contrast
Macura

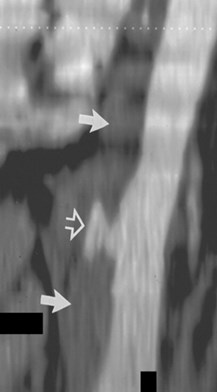
Saccular aneurysm of arch caused by penetrating ulcer, unenhancedshows aneurysm with thrombus and IMH, enhanced showsoutpouching of contrast from lumen
Castaner
Atheromatous ulcers confined to intima, only visualized aftercontrast.
Castaner
Complications
Death from thoracic aortic dissection:acute aortic insufficiency, major branchvessel obstruction, pericardialtamponade, aortic rupture
Complications of other organs: ischemiasecondary to obstruction of branchvessels such as renal arteries withinfarction in kidneys

Rupture ofpenetrating ulcerwith acutemediastinalhematoma andhemothorax
Castaner
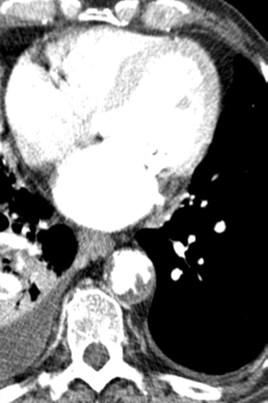
Rupture of Type A aorticdissection with stenosis ofpulmonary arteries which areenveloped in hemorrhage
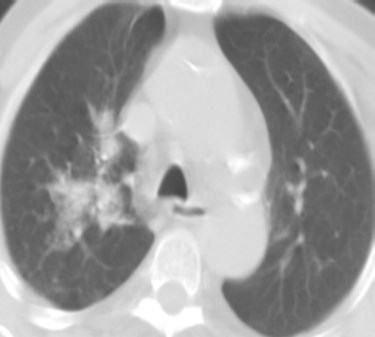
Alveolar opacity caused byblood dissecting aroundbronchovascular bundles
Castaner
Rupture of Type A dissection along pulmonary arteries withluminal narrowing
Castaner


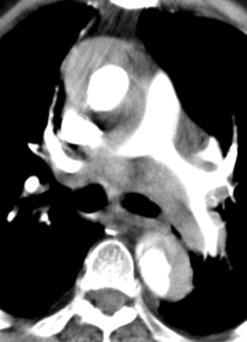
True lumen of celiac trunk and left renal artery narrowed bythrombosed false lumen. Left renal infarction
Castaner
References
Castaner E, etal. CT in Nontraumatic Acute Thoracic AorticDisease: Typical and Atypical Features and Complications.RadioGraphics 2003;23:S93-S110
LePage MA, etal. Aortic Dissection: CT Features thatDistinguish True from Flase Lumen. AJR 2001; 177:207-211
Macura KJ, etal. Pathogenesis in Acute Aortic Syndromes:Aortic Dissection, Intramural Hematoma, and PenetratingAtherosclerotic Aortic Ulcer. AJR 2003; 181:309-316
Sueyoshi E. New Development of an Ulcerlike Projection inAortic Intramural Hematoma: CT Evaluation. Radiology2002;224:536-541
The End